Melancholic depression has long resisted the explanatory schemes that govern reactive psychopathology. Clinicians can often trace the symptoms of grief, post-traumatic disorder, or adjustment reaction to identifiable precipitants in the patient’s recent history; the same operation routinely fails when applied to the deeper varieties of depressive illness, those that classical European psychiatry termed endogen, those that the Newcastle Group of the 1960s catalogued under the rubric of “no adequate psychogenesis,” and those that DSM-5 retains, with some terminological circumlocution, in its melancholic specifier.(1) The clinical observation that the patient suffering from such an episode cannot identify a trigger, and that the clinician, even after extended interview, cannot supply one in lieu of the patient’s failure, has typically been received either as evidence of poor insight on the patient’s part, requiring further interpretive work to recover a suppressed precipitant, or as a methodological artefact arising from the limitations of recall, the suggestibility of self-report, and the inherent vagueness of the stress concept itself.(2) Both readings miss the structural significance of the observation.
The cause of melancholic depression is an integrated quantity, a global feature of the patient’s life-trajectory whose value depends on the area enclosed by that trajectory and not on any particular point along it. Holonomy, the residual rotation accumulated by a vector that has been parallel-transported around a closed loop on a curved manifold, is its formal name. The patient’s inability to identify a trigger and the clinician’s inability to extract one are accurate first- and third-person reports of a causal grain that lies at the level of the integral and not at the level of the moment.(3)
I. Mathematical preliminaries
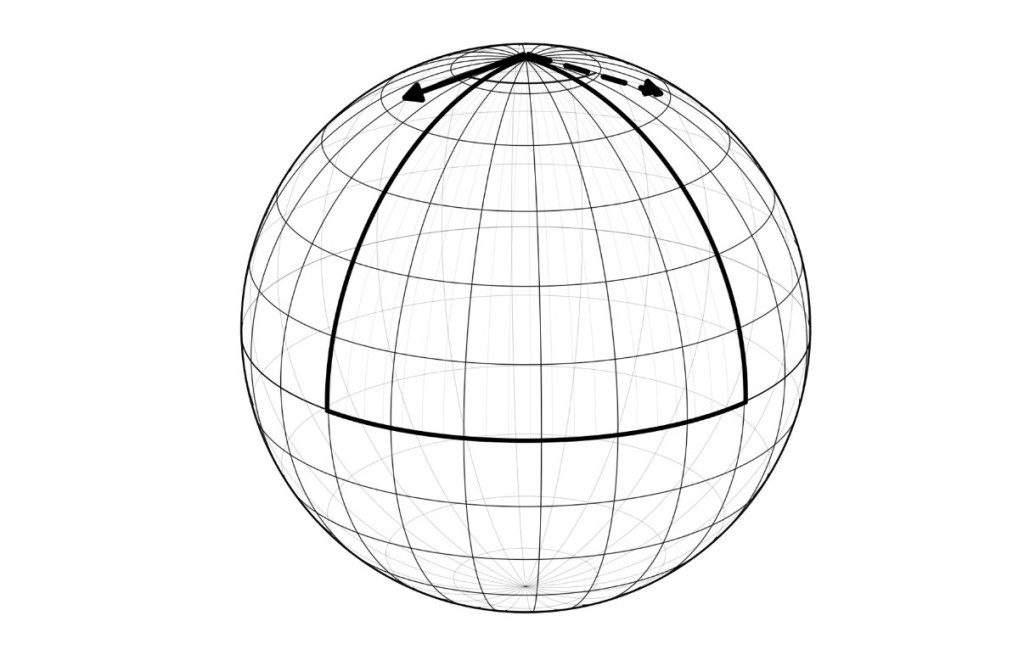
Take a unit sphere, the standard S² of mathematical convention, and a vector situated at the north pole, pointing along an arbitrarily chosen meridian. Parallel transport requires that this vector be carried along a curve in such a way that, at each point of the curve, it remains “as parallel to itself as possible,” in a sense the geometry of the sphere defines precisely. Suppose the vector is carried south along its meridian to the equator, then east along the equator through ninety degrees of longitude, then north along the new meridian back to the pole. Upon arrival, the vector, which has been held as motionless as the sphere permitted at every step of the journey, points in a direction rotated through a right angle from its starting direction. The rotation is not the result of any local operation on the vector. At no point during the transport was the vector turned, twisted, or otherwise acted upon. The rotation is a global feature of the loop, equal to the integral of the sphere’s Gaussian curvature over the spherical triangle the path enclosed.(4)
The phenomenon is general. On any Riemannian manifold (M, g), the metric g uniquely determines an affine connection ∇, the Levi-Civita connection, by the requirement that ∇ be both compatible with the metric (so that lengths and angles are preserved under transport) and torsion-free (so that no spurious twist is introduced beyond what the curvature dictates).(5) Given this connection, a vector field V along a curve γ:[a,b] → M is parallel-transported along γ if the covariant derivative ∇_γ̇V vanishes identically. For each closed loop γ at a point p ∈ M, parallel transport defines a linear map P_γ: T_p M → T_p M, which, by virtue of the metric compatibility of the connection, is necessarily an isometry of the tangent space. The set of all such maps, as γ ranges over the closed loops at p, forms a Lie subgroup of the orthogonal group, the holonomy group of the connection at p.(6)
For oriented two-dimensional surfaces, the holonomy group is contained in SO(2), and parallel transport around any sufficiently small closed loop is a rotation through some angle θ. The Gauss–Bonnet theorem, in its local form, gives this angle: θ equals the integral of the Gaussian curvature K over the region D enclosed by the loop, modulo 2π.(7) On a geodesic triangle, a triangle whose sides are geodesics, like the spherical triangle just considered, the theorem reduces to the angular-excess formula: the sum of the interior angles minus π equals ∫∫_T K dA. The right-angled triangle on the unit sphere yields an excess of π/2, an enclosed area of π/2 (since the triangle is one-eighth of a sphere of total area 4π), and an integrated curvature of π/2, in agreement with the rotation observed in the parallel-transport calculation.
The vector’s rotation is independent of how fast it was transported, of what particular sequence of points it passed through, of the local curvature at any specific point of the trajectory; it depends only on the integral of the curvature over the region the loop enclosed. The curvature tensor itself is a local object, defined pointwise on the manifold; the holonomy is global. The Ambrose–Singer theorem makes the relation precise: the Lie algebra of the holonomy group at p is generated by the values of the curvature 2-form at all points horizontally accessible from p, while the holonomy itself is not equal to any pointwise quantity, and cannot be read off from any local inspection of the path.(8) On a closed orientable surface, the integral of the Gaussian curvature is fixed by the topology, equal, by the global Gauss–Bonnet theorem, to 2π χ(M), where χ(M) is the Euler characteristic, and is invariant under any continuous deformation of the metric. Pointwise curvature can be redistributed across the surface by such deformation; the integral cannot.
A Foucault pendulum suspended at colatitude θ₀ on the rotating earth has its plane of oscillation parallel-transported once around the latitude circle in the course of a sidereal day. The plane returns rotated through an angle of 2π(1 − cos θ₀), which equals the solid angle subtended by the spherical cap above the latitude circle, which equals, by Gauss–Bonnet on the unit sphere, the integral of the Gaussian curvature over that cap.(9) The Coriolis force, which implements the parallel transport at every instant, is conservative; the rotation of the plane is the global residue of having traversed the closed loop. A charged particle traversing a region in which the magnetic field is identically zero, but which encloses a confined magnetic flux, accumulates a quantum-mechanical phase shift equal to (q/ℏ) times the enclosed flux; the Aharonov–Bohm effect appears along a trajectory at every point of which the local field is zero.(10) A quantum system held in an instantaneous eigenstate while its parameters are slowly varied around a closed loop in parameter space acquires Berry’s geometric phase, dependent on the area enclosed in parameter space and weighted by the Berry curvature, independent of the rate at which the loop is traversed.(11) Berry himself classified these phenomena under the heading of anholonomy, “global change without local change.”(12)
II. The structural thesis
Mood functions as a connection on the manifold of lived experience. Mood is the structural condition that determines how affective states are carried from moment to moment, what counts as the “same” affect at different points in time, what counts as a return to a previous orientation. Mood is the rule that determines parallel transport, the rule by which yesterday’s affect is carried into today’s, the rule that decides whether a given Tuesday morning is “infinitesimally parallel” to the Monday evening that preceded it. Heidegger’s Stimmung, Blankenburg’s Selbstverständlichkeit, Fuchs’s implicit-temporal attunement, and Ratcliffe’s existential feeling articulate the same structural-disclosive character of mood.(13)
Affective states are tangent vectors at points on the manifold of lived experience. A particular sadness, joy, irritation, or longing is, at each moment of its occurrence, a specific vector at a specific point of the lived trajectory, with both a direction (its intentional or quasi-intentional orientation toward the world) and a magnitude (its felt intensity). The transport of such vectors through time is governed by the connection that mood constitutes. Two moments of “feeling worried about X,” when X is the same and the worry is comparably intense, may yet be infinitesimally non-parallel relative to the connection in force; the difference between them lies in the local geometry that decides what counts as the same vector at different points. The same affective content at different times can stand in non-trivial geometric relation to itself, and depression is the cumulative manifestation of that non-triviality.
Depression is the holonomy of the mood-connection around a closed loop of cyclical time. The natural cycles of human life (the day, the week, the month, the season) trace closed loops on the manifold of lived experience. Affect, parallel-transported along these loops by the mood-connection, accumulates a residual rotation whose magnitude depends on the integrated curvature enclosed. When the curvature integral over the region the loop encloses is below a threshold, affect returns approximately to itself: one wakes the morning of one Monday roughly oriented as one was the previous Monday, and the cycles of life close upon themselves in a way that permits ordinary life to continue. When the integral exceeds the threshold, the rotation is large enough that affect no longer aligns with its starting orientation. The world, met by an affect-vector that points in a direction it did not previously point, presents itself as different, distant, or unreachable, because the angle from which it is met has been altered. Depression is the topological invariant produced when the misalignment occurs and persists.
The geometry is rotation rather than magnitude reduction. Clinical descriptions of melancholic depression repeatedly emphasize that the patient is differently oriented, not less affective in the manner of someone exhausted, but, that the world has somehow been changed in a way that no event changed it.(14) The cause is integrated, area-distributed, and global, no less causal for being structurally irreducible to any local stimulus. The depressive episode is the residue of cumulative history, the integral of curvature traversed.
III. The phenomenological tradition
Heidegger’s Stimmung
Stimmung, in Heidegger’s development of the term in Sein und Zeit §§29–30 on Befindlichkeit and §40 on Angst, is the disclosedness in which feeling-about-something becomes possible: “The mood has already disclosed, in every case, Being-in-the-world as a whole, and makes it possible first of all to direct oneself towards something.”(15) The disclosure is prior to any encounter with a specific worldly entity; the very possibility of such an encounter presupposes the disclosure that mood has already accomplished. Befindlichkeit, the condition of finding oneself in a mood, has the same structural character that a connection has on a Riemannian manifold: the rule by which the world is given its overall shape, the prior condition that determines what can subsequently appear within it.
Angst, in §40, has no specific intentional object; it is anxiety-about, but not anxiety about this or that particular being. “That in the face of which one is anxious is completely indefinite.”(16) What anxiety reveals is world itself, an alteration of the connection rather than of any vector being transported by it. Tiefe Langeweile, profound boredom, treated in Die Grundbegriffe der Metaphysik (1929–30) as a fundamental mood (Grundstimmung), exhibits the same lack of any particular object: “Profound or fundamental boredom is that which is not related to any particular being, but beings as a whole.”(17) The withdrawal is global, a re-shaping of the field within which encounters take place.
Blankenburg and the loss of natural self-evidence
Grundstörung, the basal disturbance Blankenburg theorized in Der Verlust der natürlichen Selbstverständlichkeit (1971), is a loss of the unreflective givenness of everyday life, natürliche Selbstverständlichkeit, “natural self-evidence.”(18) The patient cannot point to what has gone wrong because what has gone wrong is the precondition for anything to be given as taken-for-granted in the first place. Blankenburg’s patient Anne Rau testifies repeatedly: “What is it that I really lack? Something so small, but so peculiar, something so important, without it one cannot live… It is simply Selbstverständlichkeit that I lack.”(19) The disturbance is at the field-condition, not at any object within the field.
Fuchs and desynchronisation
Desynchronisation, in Thomas Fuchs’s account, is the cumulative misalignment between the implicit time of the body (its rhythms, its tacit operative attunement) and the explicit time of the social environment.(20) “Melancholia,” he writes, “is then interpreted as the result of a desynchronization, i.e. an uncoupling in the temporal relation of organism and environment, or of individual and society. With the processes of resynchronization failing, the person falls out of common environmental time.”(21) Desynchronisation is, by construction, an integrated quantity, the sum of small temporal mismatches accumulated over many cycles of bodily and social rhythm. The melancholic does not desynchronise at any particular moment; the accumulated misalignment crosses a threshold beyond which the implicit synchrony that ordinarily holds the patient in the social fabric can no longer be maintained. The “corporealization” of the lived body, its becoming material and impeding rather than transparent and operative in the language of Husserl’s Leib/Körper distinction, is the felt manifestation of accumulated holonomy.(22)
Kimura and the post festum
Post festum, in Kimura Bin’s festum theory, is the temporal mode of the always-already-too-late, oriented toward a past that exceeds any possible reparation.(23) In Kimura’s typology, schizophrenia stands under the temporal mode of ante festum (the perpetually anticipatory, oriented toward a future that never arrives), while melancholia stands under post festum. The melancholic, on Kimura’s account, “must feel that they could not achieve order and that they were ‘late for themselves’ because of ‘having done irrecoverable actions’… these patients live in the perfect tense.”(24) The depressive’s relation to the past is to a generalized lateness, a structural debt that exceeds any specific obligation. The patient cannot identify what they are too late for because the lateness is integrated over the entire trajectory and has no specific past event as its referent.
Tellenbach’s typus melancholicus
The typus melancholicus, the premorbid character that, on Tellenbach’s account in Melancholie (1961), predisposes to melancholic illness, is characterized by Includenz (the self-contradiction whereby the typus melancholicus simultaneously maintains and exceeds his order) and Remanenz (the danger of remaining behind regarding one’s own expectations and the emergency of the duty).(25) The typus melancholicus, Tellenbach argues, “is conditioned by the paradoxical tendency of cancelling possible debts in advance,” producing over time a cumulative pressure of unmet self-imposed obligation that no specific day’s labour can ever fully discharge. The depressive emerging from this premorbid type is the integrated effect of an accumulated debt of expectation that builds over many cycles of conscientious self-application. The Goethean morphological framework underlying Tellenbach’s endon (the inner principle of melancholic susceptibility) treats the disposition as a process of substantial transformation across time.(26)
Ratcliffe and existential feeling
Existential feeling, in Matthew Ratcliffe’s articulation across Feelings of Being (2008) and Experiences of Depression (2015), is a “felt sense of belonging to the world,” prior to and conditioning of any object-directed feeling.(27) Depression, for Ratcliffe, is a re-shaping of the very space of possibilities the world offers: “one not only loses however many actual hopes but also an orientation that is presupposed by the possibility of hoping for anything.”(28) The orientation that is presupposed by the possibility of hoping is the connection that determines parallel transport; its alteration is a re-determination of how the lived field is given. Ratcliffe’s testimony reports, “It is like falling into a deep black pit… a state of nonbeing”; “I awoke into a different world. It was as though all had changed while I slept”; “I felt like I’d been found incompetent and fired from my own life,”(29) describe a world no longer given as it was.
IV. The clinical literature
Diagnostic recognition of mood unreactivity
Kraepelin, in Manic-Depressive Insanity and Paranoia (1921), described episodes that arose without apparent external cause and that progressively accelerated with successive recurrences.(30) Vitalgefühl, the term Kurt Schneider isolated as the felt-quality of vital sadness characteristic of endogenous depression, names a sadness that does not respond to ordinary positive stimuli and that exhibits diurnal variation, early-morning awakening, and psychomotor change.(31) The Newcastle Diagnostic Scale, developed by Carney, Roth, and Garside in 1965, codified these features into a ten-item scale, the second item of which, “no adequate psychogenesis,” identified the absence of psychological stress sufficient to explain the illness as a positive diagnostic feature.(32) Absence of trigger entered the diagnostic apparatus as a sign in its own right.
Donald Klein’s 1974 concept of endogenomorphic depression defined the condition as “a sharp, unreactive, pervasive impairment of the capacity to experience pleasure, or to respond affectively, to the anticipation of pleasure.”(33) The unreactivity to local positive stimuli, the failure of mood to lift when something good happens, became the operational basis for the DSM’s melancholic specifier, which retains the formulation as Criterion A2: “lack of mood reactivity to usually pleasurable stimuli.”(34) DSM-5-TR clarifies that the criterion is met “only when there is a near-complete absence of the capacity for pleasure, not merely a diminution.” ICD-11 retains the same core distinction in its “with melancholia” specifier, with criteria parallel to those of DSM-5.(35)
Empirical prevalence of episodes without identifiable precipitant
Brown, Harris, and Hepworth’s 1994 study using the Life Events and Difficulties Schedule (LEDS), the gold-standard interview-based measure of severe stressors, found that 60% of recurrent melancholic-psychotic episodes occurred without any severe life event in the preceding period, compared with 27% of non-melancholic episodes.(36) The figure is consistent with earlier work by Frank and colleagues, who reported approximately 57% of RDC-defined endogenous depressions without identified stressors over six months.(37) The absence of identifiable precipitants is most pronounced in recurrent rather than first episodes; first endogenous episodes were more often associated with stressors than recurrences in the Brown sample, indicating a course-dependent decoupling of clinical state from life-event stimulus. The LEDS is a structured contextual interview designed to detect severe life events that less rigorous instruments would miss; the 60% figure reflects episodes occurring in the absence of any severe stressor that careful interview can disclose. Parker’s Sydney Melancholia Prototype Index includes, as a positive diagnostic item, the patient’s own characterization of the episode as occurring “out of the blue,” with reported sensitivity of 0.84 and specificity of 0.92 against clinician judgement of melancholic status.(38)
The kindling hypothesis
Kindling, the framework Robert Post advanced in 1992 by analogy with amygdala kindling in animal models and with stimulant sensitization in addiction, posits that recurrent affective illness exhibits two parallel sensitization processes: an episode sensitization (in which the well intervals between successive episodes shorten and the threshold for episode emergence falls) and a stress sensitization (in which the magnitude of psychosocial stressor required to trigger an episode declines with each recurrence).(39) Post predicts the transition from triggered to autonomous episodes: “the model presents a clear-cut example of the shift from episodes that are triggered to those that occur autonomously,” with later episodes occurring with “less and less of an environmental contribution.”(40)
Kendler, Thornton, and Gardner’s 2000 twin-pair analysis of 2,395 female-female twin pairs over 97,515 person-months and 1,380 onsets demonstrated a progressive decline in the strength of the stressful-life-event–major-depression association as a function of prior episode count, with the association stabilizing only after roughly nine prior episodes.(41) Stroud, Davila, and Moyer’s 2008 meta-analysis replicated and refined the finding, although the model remains contested on the precise course of cycle acceleration.(42) Life-event triggers progressively cease to predict depressive recurrence as the disorder develops; the integrated history of prior episodes rather than any present input becomes the predominant determinant of depressive state. The Kendlerian “prekindling” finding, that individuals at high genetic risk show the weak-stress association already at first episode, equivalent to the third-episode pattern in low-risk individuals, extends the integrated-history model to apparently first episodes in genetically vulnerable patients.(43)
Allostatic load
Allostatic load, the term McEwen and Stellar introduced in 1993 by extending Sterling and Eyer’s 1988 allostasis (“stability through change”), is the cumulative wear-and-tear on the body that results from chronic activation of allostatic mediators.44 McEwen’s 1998 articles in the New England Journal of Medicine and the Annals of the New York Academy of Sciences developed the framework: “It is not just the dramatic stressful events that exact their toll, but rather the many events of daily life that elevate and sustain activities of physiological systems and cause sleep deprivation, overeating, and other health-damaging behaviors, producing the feeling of being ‘stressed out.’ Over time, this results in wear and tear on the body, which is called ‘allostatic load.’”(45)
Allostatic load is a time-integral of mediator activation, accumulated across small daily challenges that individually fail to register as discrete events. The pathology emerges when the integral crosses a threshold, not when any particular stressor occurs. Kanner and Lazarus’s 1981 work on “daily hassles” had anticipated the finding at the psychological level: their 117-item Hassles Scale, administered monthly to middle-aged adults over nearly a year, “was a better predictor of concurrent and subsequent psychological symptoms than were the life events scores,” with the predictive power remaining significant after the variance attributable to discrete life events was controlled.(46)
Prolonged glucocorticoid exposure damages hippocampal CA3 neurons that ordinarily provide negative feedback to the hypothalamic-pituitary-adrenal (HPA) axis, producing a positive-feedback runaway in which the system’s response to subsequent stressors decouples from the magnitude of those stressors and becomes dependent on the cumulative history of prior activation.(47) The dependence on history rather than on current input is documented in hippocampal volume changes, in operationally defined biomarker indices, and in dose-dependent relationships between cumulative stress exposure and depression risk.
Prodromal continuity
Fava and Kellner’s 1991 study found that all 15 first-episode patients in their initial sample reported at least one prodromal symptom prior to depressed mood, with anxiety, irritability, and impaired initiative typically appearing months before clinical diagnosis.(48) The 2024 DEEP-IN cohort study by Höhn and colleagues found prodromal phases in 93.2% of remitted patients, with a mean duration of 7.9 months (SD 12.5).(49) An Indian replication found prodromal symptoms in 100% of 80 remitted patients, with a mean duration of 115 days. “Episode onset” at the moment of diagnostic interview is a sampling artefact, the moment at which a continuously developing process crosses the diagnostic threshold. There is the integral, observed at the point at which it can no longer be ignored. The clinical search for a triggering event in the period immediately prior to diagnosis is searching for an arbitrary point on a long preceding curve, a point whose features are uninformative about the curve’s overall shape.
V. The category error of the trigger-search
To ask “what triggered this episode” presupposes that depression is a punctate response to a discrete antecedent stimulus, and that the cause of the episode should therefore be locatable at some specific point in the patient’s recent history. The presupposition that depression is a state-variable updated by punctate events conflicts with the diagnostic-criterial recognition of mood unreactivity (Klein, DSM-5 Criterion A2, ICD-11 melancholic specifier), with the empirical prevalence of episodes without identifiable precipitants (Brown, Frank), with the kindling phenomenon (Post, Kendler), and with the phenomenological claim that mood is a structural-disclosive condition (Heidegger, Ratcliffe, Fuchs). The presupposition that the cause should be locatable at a specific point conflicts with what holonomy is: an area-quantity computed over the region the loop encloses, with no point-location. The patient’s report that “I don’t know why” is an accurate first-person description of where the cause is.
A category error, on the standard usage, occurs when the predicates appropriate to one ontological category are applied to another, as when one asks for the colour of a number or the weight of a virtue. The clinical question “what triggered this episode,” posed of melancholic depression, asks for a property (locatability at a specific past moment) that the phenomenon does not possess. What is the curvature distribution over the region of life the loop has enclosed; what is the integrated trajectory of the patient’s allostatic exposure, premorbid disposition, and previous episode history; what condition of the mood-connection is currently in force, and what would change it: none of these questions admits of a punctate answer.
Pharmacological treatment of depression already operates at the level of the integral. Selective serotonin reuptake inhibitors and tricyclic antidepressants exert their clinical effects only after weeks of administration, during which the molecular changes at receptor and post-receptor levels integrate to a structural alteration of monoaminergic tone and downstream effects on hippocampal neuroplasticity.(50) Antidepressant response requires sustained administration over weeks; no particular dose or moment produces the response.
Cognitive-behavioural therapy is founded on the proposition that depression is sustained by identifiable maladaptive thoughts whose modification will lift the depression. The model requires a tight coupling of present cognition to present mood. Parker and colleagues’ 2013 randomized controlled trial showed antidepressant medication superior to CBT in melancholic patients across a 12-week course, with the superiority most pronounced in the patients with the most prototypical melancholic features.(51) Teasdale and Fennell had shown, in 1987, that distraction techniques, which depend on the same thought-mood causal coupling Beck’s cognitive theory postulates, did not significantly alter depressed mood in patients high on the Newcastle endogenous score.(52) One cannot relieve holonomy by adjusting the local features of the path; the local features are not what produced the rotation.
Therapeutic strategies that operate on the integral include sleep and circadian-rhythm modifications, chronotherapeutic interventions, exercise pursued as a sustained rather than episodic practice, dietary and metabolic interventions whose effects accumulate over weeks, and contemplative practices that aim at modification of the connection itself. The proper measure of therapeutic progress in melancholic illness is the change in the integrated trajectory across many days, a measure that current outcome instruments, with their typical reliance on point-in-time symptom inventories, capture only imperfectly.
Conclusion
The patient who cannot identify a trigger and the clinician who cannot find one are reporting accurately on a phenomenon whose causal grain is the integral and not the moment. The phenomenological tradition since Heidegger has identified mood as a structural-disclosive condition rather than an object-directed feeling; the clinical tradition since Kraepelin has identified melancholic illness as autonomous from current stimulus; differential geometry, in connections and parallel transport, provides the structural vocabulary for what both traditions describe.
The substrate of the holonomic structure in the human case is the cumulative trajectory of HPA-axis sensitization, hippocampal-prefrontal feedback dysregulation, circadian and chronobiological dysrhythmy, and the integrated metabolic and inflammatory consequences of allostatic load. Each accumulates by integration. The clinical question that searches, in melancholic depression, for the discrete antecedent of an integrated phenomenon asks for a property the phenomenon does not possess.
Footnotes
- On the historical development of the endogenous-reactive distinction, see Carney, Roth and Garside, “The diagnosis of depressive syndromes and the prediction of E.C.T. response,” Br J Psychiatry 111 (1965) 659–74; Klein, “Endogenomorphic depression: a conceptual and terminological revision,” Arch Gen Psychiatry 31 (1974) 447–54; Parker and Hadzi-Pavlovic (eds.), Melancholia: A Disorder of Movement and Mood (Cambridge University Press, 1996); Shorter and Fink, Endocrine Psychiatry (Oxford University Press, 2010). For the historiography of the DSM-III collapse of categorical endogenous-reactive into unitary MDD with melancholic specifier, see Klerman, Endicott, Spitzer and Hirschfeld, “Neurotic depressions: a systematic analysis,” Am J Psychiatry 136 (1979) 57–61; Kendell, “The classification of depressions,” Br J Psychiatry 129 (1976) 15–28.
- For the “poor insight” reading and its problems, see Ghaemi, “Insight and psychiatric disorders: a review of the literature, with a focus on its clinical implications for bipolar disorder,” PMC2632297, who notes that depressed patients are typically more insightful than manic ones, undercutting any simple insight-deficit reading. For the methodological-artefact reading, see Monroe and Reid, “Gene-environment interactions in depression research,” 947–56; for the rebuttal from the LEDS-based literature, see Brown, Harris and Hepworth, Br J Psychiatry (cited in n. 36 below).
- On the relationship between structural and mechanistic accounts in the philosophy of psychiatry, see Kendler, “Toward a philosophical structure for psychiatry,” Am J Psychiatry 162 (2005) 433–40; Borsboom et al., “A network theory of mental disorders,” Annual Review of Clinical Psychology 9 (2013) 91–121.
- The example is standard in the differential geometry textbook tradition; see do Carmo, Differential Geometry of Curves and Surfaces (Prentice-Hall, 1976), §4.4; Spivak, A Comprehensive Introduction to Differential Geometry (Publish or Perish, 1979), vol. II, ch. 6.
- For the existence and uniqueness of the Levi-Civita connection (the “Fundamental Theorem of Riemannian Geometry”), see do Carmo, Riemannian Geometry (Birkhäuser, 1992), §2.3, Theorem 3.6; Lee, Riemannian Manifolds: An Introduction to Curvature (Springer, 1997), Theorem 5.4; Kobayashi and Nomizu, Foundations of Differential Geometry, vol. I (Wiley, 1963), §III.3. The Koszul formula for the connection in coordinate-free terms is given in do Carmo, Riemann Ian Geometry, §2.3.
- For the holonomy group, see Kobayashi and Nomizu, Foundations, vol. I, §II.4; Lee, Riemannian Manifolds, ch. 7; Nakahara, Geometry, Topology, and Physics (Institute of Physics, 2003), §7.3. For Berger’s classification of irreducible Riemannian holonomy groups, see Berger, “Sur les groupes d’holonomie homogène des variétés à connexion affine et des variétés riemanniennes,” Bull. Soc. Math. France 83 (1955) 279–330; Joyce, Riemannian Holonomy Groups and Calibrated Geometry (Oxford University Press, 2007), ch. 3.
- For the local Gauss–Bonnet theorem, see do Carmo, Differential Geometry, p. 268 and p. 274 (for the global version); Spivak, Comprehensive Introduction, vol. II, ch. 6. For the angular-excess interpretation, see do Carmo, Differential Geometry, Corollary 4.
- Ambrose and Singer, “A theorem on holonomy,” Trans AMS 75 (1953) 428–43; Kobayashi and Nomizu, Foundations, vol. I, p. 89.
- For the Foucault pendulum as an instance of holonomy, see Hannay, “Angle variable holonomy in adiabatic excursion of an integrable Hamiltonian,” J Phys A 18 (1985) 221–30; Berry, “Anticipations of the geometric phase,” Physics Today 43:12 (1990) 34–40; Stoytchev, “The geometric phase of the Foucault pendulum,” arXiv:1701.01666 (2017).
- Aharonov and Bohm, “Significance of electromagnetic potentials in quantum theory,” Phys Rev 115 (1959) 485–91; for experimental confirmation with shielded toroidal magnets, see Tonomura et al., “Evidence for Aharonov-Bohm effect with magnetic field completely shielded from electron wave,” Phys Rev Lett 56 (1986) 792–95.
- Berry, “Quantal phase factors accompanying adiabatic changes,” Proc Roy Soc A 392 (1984) 45–57; Simon, “Holonomy, the quantum adiabatic theorem, and Berry’s phase,” Phys Rev Lett 51 (1983) 2167–70.
- Berry, CERN lectures on geometric phases, AT00000125 (1996), p. 1. The terminological choice between “holonomy” and “anholonomy” is largely a matter of emphasis; the latter highlights the failure of variables to return to their initial values after a closed loop, the former highlights the structure governing the failure.
- For Befindlichkeit in Husserl, see Ideen I, §50, on the affective-tonal dimension of the natural attitude; the concept is taken up and developed in Ideen II §§35–42 on the Leib-Körper distinction.
- Stanghellini and Rosfort, Emotions and Personhood: Exploring Fragility – Making Sense of Vulnerability (Oxford University Press, 2013), ch. 4; Sass and Pienkos, “Faces of intersubjectivity: a phenomenological study of interpersonal life in melancholia, mania, and schizophrenia,” Journal of Consciousness Studies 20 (2013) 131–52.
- Heidegger, Sein und Zeit (Niemeyer, 1927); English trans. Macquarrie and Robinson, Being and Time (Blackwell, 1962), p. 176/SZ p. 137.
- Being and Time, §40, p. 231/SZ p. 186; cf. Was ist Metaphysik?: “Anxiety reveals the nothing,” in Krell (ed.), Basic Writings (Harper, 1977), p. 103.
- Heidegger, Die Grundbegriffe der Metaphysik (GA 29/30), lectures of 1929–30, English trans. McNeill and Walker, The Fundamental Concepts of Metaphysics (Indiana University Press, 1995), §28; on the Grundstimmung of profound boredom, see also Stolorow, “Heidegger and post-Cartesian psychoanalysis,” Janus Head 8:1 (2005) 211–14.
- Blankenburg, Der Verlust der natürlichen Selbstverständlichkeit: Ein Beitrag zur Psychopathologie symptomarmer Schizophrenien (Enke, 1971; Parodos, 2012); partial English translation in Mishara, “First steps toward a phenomenology of common sense,” Philosophy, Psychiatry, and Psychology 8 (2001) 303–15.
- Quoted in Mishara, “First steps,” p. 308; the German original appears in Blankenburg, Verlust, p. 67.
- Fuchs, Ecology of the Brain (Oxford University Press, 2018); “Melancholia as a desynchronization: Towards a psychopathology of interpersonal time,” Psychopathology 34 (2001) 179–86; “Temporality and psychopathology,” Phenomenology and the Cognitive Sciences 12 (2013) 75–104; “Corporealized and disembodied minds: a phenomenological view of the body in melancholia and schizophrenia,” Philosophy, Psychiatry, and Psychology 12 (2005) 95–107.
- Fuchs, “Melancholia as a desynchronization,” p. 179.
- Fuchs, “Corporealized and disembodied minds,” pp. 99–101; the Husserlian Leib/Körper distinction is treated in Ideen II, §§35–42; for its application in clinical phenomenology, see Stanghellini, Disembodied Spirits and Deanimated Bodies: The Psychopathology of Common Sense (Oxford University Press, 2004).
- Kimura, Aida (Kobundo, 1988); Hito to hito to no aida (Kobundo, 1972); Écrits de psychopathologie phénoménologique, French trans. with postface by Maldiney (Presses Universitaires de France, 1992).
- Kimura, Écrits, cited in Fukao (2023) and Noma (2023); Agamben’s discussion of post festum in The Omnibus Homo Sacer, pp. 1287–92.
- Tellenbach, Melancholie: Problemgeschichte, Endogenität, Typologie, Pathogenese, Klinik (Springer, 1961; expanded eds. 1974, 1976, 1983); English trans. Eng, Melancholy (Duquesne University Press, 1980); Stanghellini and Bertelli, “Assessing the social behaviour of typus melancholicus,” Psychopathology 39 (2006) 179–85.
- The Goethean morphological framework underlying Tellenbach’s endon concept is developed at length in Melancholy, ch. 7; on the reception of the concept in subsequent clinical phenomenology, see Englebert and Stanghellini, “Typus melancholicus and melancholia: theoretical synthesis using a clinical case,” Annales Médico-Psychologiques (2010).
- Ratcliffe, Feelings of Being: Phenomenology, Psychiatry, and the Sense of Reality (Oxford University Press, 2008); Experiences of Depression: A Study in Phenomenology (Oxford University Press, 2015).
- Ratcliffe, Experiences of Depression, p. 109; cf. p. 72: “It is not just that one’s belief contents change; the way in which one believes changes too.”
- Ratcliffe, Experiences of Depression, ch. 3, drawing on memoirs collected in Whybrow, A Mood Apart (HarperCollins, 1997), p. 23; Rowe, The Experience of Depression (Wiley, 1978), pp. 268–70; Steinke (2001), p. 64.
- Kraepelin, Manic-Depressive Insanity and Paranoia, English trans. Barclay, ed. Robertson (Livingstone, 1921), particularly the discussion of episode acceleration on pp. 142–58.
- Schneider, Klinische Psychopathologie, 5th ed. (Thieme, 1950), pp. 81–95.
- Carney, Roth and Garside, “The diagnosis of depressive syndromes,” 659–74; Kiloh and Garside, “The independence of neurotic depression and endogenous depression,” Br J Psychiatry 109 (1963) 451–63; Kay et al., “Endogenous and neurotic syndromes of depression: a 5- to 7-year follow-up of 104 cases,” Br J Psychiatry 115 (1969) 377–88.
- Klein, “Endogenomorphic depression,” p. 447.
- American Psychiatric Association, Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (American Psychiatric Publishing, 2013); DSM-5-TR (2022); Fried et al., “The 341,737 ways of qualifying for the melancholic specifier,” Lancet Psychiatry (2020).
- World Health Organization, International Classification of Diseases, 11th rev. (WHO, 2019); the “with melancholia” specifier criteria are detailed in the Clinical Descriptions and Diagnostic Guidelines.
- Brown, Harris and Hepworth, “Life events and endogenous depression,” Arch Gen Psychiatry 51 (1994) 525–34.
- Frank et al., cited in Parker, “Defining melancholia: the primacy of psychomotor disturbance,” Acta Psychiatrica Scandinavica 115 (2007) 21–30.
- Parker, McCraw, Blanch, Hadzi-Pavlovic, Synnott and Rees, “Discriminating melancholic and non-melancholic depression by prototypic clinical features,” Journal of Affective Disorders 144 (2013) 199–207; Parker, Fink, Shorter, Taylor, Akiskal, Berrios, Bolwig et al., “Issues for DSM-5: Whither Melancholia?” Am J Psychiatry 167 (2010) 745–47, PMC3733615.
- Post, “Transduction of psychosocial stress into the neurobiology of recurrent affective disorder,” Am J Psychiatry 149 (1992) 999–1010.
- Post, “Transduction,” p. 1001; Post, “Kindling and sensitization as models for affective episode recurrence, cyclicity, and tolerance phenomena,” Neuroscience and Biobehavioral Reviews 31 (2007) 858–73.
- Kendler, Thornton and Gardner, “Stressful life events and previous episodes in the etiology of major depression in women: an evaluation of the ‘kindling’ hypothesis,” Am J Psychiatry 157 (2000) 1243–51.
- Stroud, Davila and Moyer, “The relationship between stress and depression in first onsets versus recurrences: a meta-analytic review,” J Abnorm Psychol 117 (2008) 206–13; Monroe and Anderson, “Depression: the shroud of heterogeneity,” PMC4809541; Monroe and Harkness, “Life stress, the kindling hypothesis, and the recurrence of depression: considerations from a life stress perspective,” Psychological Review 112 (2005) 417–45.
- Kendler, Thornton and Gardner, “Genetic risk, number of previous depressive episodes, and stressful life events in predicting onset of major depression,” Am J Psychiatry 158 (2001) 582–86.
- McEwen and Stellar, “Stress and the individual: mechanisms leading to disease,” Arch Intern Med 153 (1993) 2093–101. Sterling and Eyer’s original formulation of allostasis appears in Fisher and Reason (eds.), Handbook of Life Stress, Cognition and Health (Wiley, 1988), pp. 629–49.
- McEwen, “Protective and damaging effects of stress mediators,” NEJM 338 (1998) 171–79; “Stress, adaptation, and disease: allostasis and allostatic load,” Annals of the New York Academy of Sciences 840 (1998) 33–44; “Protection and damage from acute and chronic stress: allostasis and allostatic overload,” Dialogues in Clinical Neuroscience 8 (2006) 367–81, PMC3181832, p. 369; Seeman, McEwen, Rowe and Singer, “Allostatic load as a marker of cumulative biological risk,” PNAS 98 (2001) 4770–75.
- Kanner, Coyne, Schaefer and Lazarus, “Comparison of two modes of stress measurement: daily hassles and uplifts versus major life events,” Journal of Behavioral Medicine 4 (1981) 1–39, p. 1; DeLongis et al., “Relationship of daily hassles, uplifts, and major life events to health status,” Health Psychology 1 (1982) 119–36.
- Sapolsky, Krey and McEwen, “The neuroendocrinology of stress and aging: the glucocorticoid cascade hypothesis,” Endocrine Reviews 7 (1986) 284–301; Lupien, McEwen, Gunnar and Heim, “Effects of stress throughout the lifespan on the brain, behaviour and cognition,” Nature Reviews Neuroscience 10 (2009) 434–45; Pariante and Lightman, “The HPA axis in major depression: classical theories and new developments,” Trends in Neurosciences 31 (2008) 464–68.
- Fava and Kellner, “Prodromal symptoms in affective disorders,” Am J Psychiatry 148 (1991) 823–30; “Staging: a neglected dimension in psychiatric classification,” Acta Psychiatrica Scandinavica 87 (1993) 225–30.
- Höhn et al., DEEP-IN cohort, Journal of Affective Disorders (2024); for the Indian replication, see PMC6058442; Iacoviello, Alloy, Abramson, Choi and Morgan, “Patterns of symptom onset and remission in episodes of depression: a 2.5-year prospective study,” PMC2916193.
- Frazer and Daws, “Slow-onset of antidepressant action,” PMC2998711; Castren, “Neurotrophic effects of antidepressant drugs,” Current Opinion in Pharmacology 4 (2004) 58–64.
- Parker, Blanch, Paterson, Hadzi-Pavlovic, Sheppard, Manicavasagar, Synnott et al., “The superiority of antidepressant medication to cognitive behaviour therapy in melancholic depressed patients: a 12-week single-blind randomised study,” Acta Psychiatrica Scandinavica 128 (2013) 271–81.
- Teasdale and Fennell, “Immediate effects on depression of cognitive therapy interventions,” Cognitive Therapy and Research 8 (1984) 343–52; Teasdale, “The effects of distraction on disturbance in clinically depressed patients,” Behaviour Research and Therapy 17 (1979) 65–74.

Leave a comment