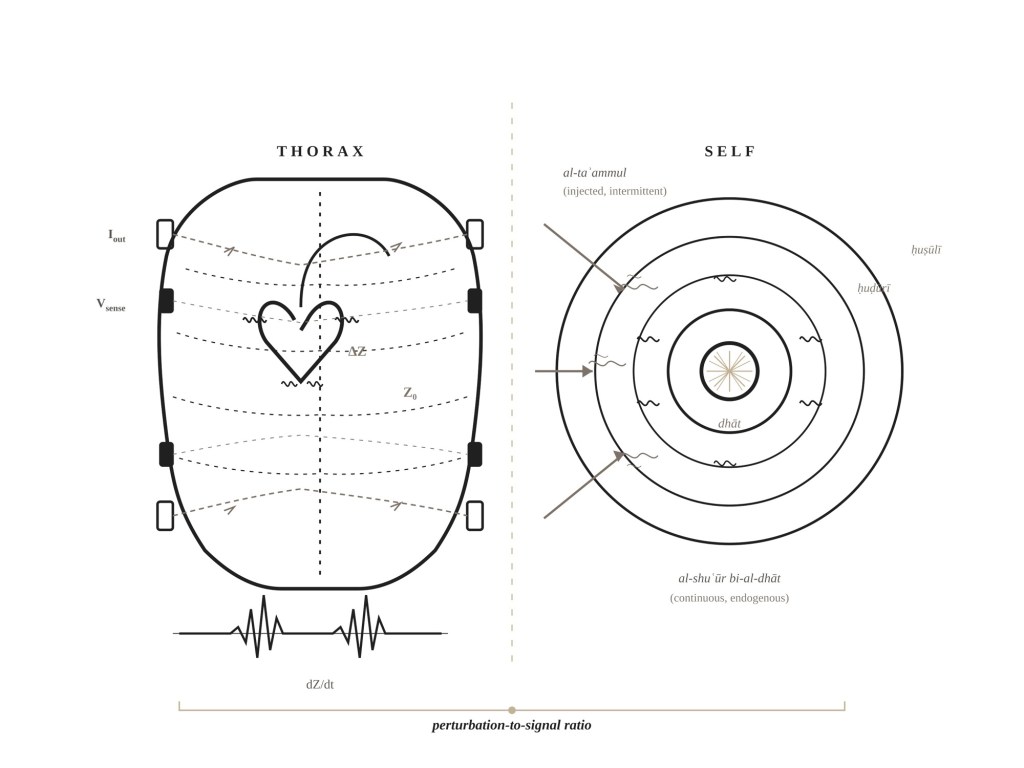
Impedance cardiography measures cardiac output by passing a small alternating current through the thorax, typically 1 to 4 milliamperes at 20 to 100 kilohertz, and measuring changes in electrical impedance as blood volume shifts with each heartbeat. Blood has lower resistivity than the tissue surrounding it: lung parenchyma, depending on air content, ranges from 200 to 5,000 ohm-centimeters; fat and bone sit higher still; blood, at roughly 100 to 150 ohm-centimeters, provides the path of least resistance through which the injected current preferentially travels, predominantly via the thoracic aorta, which accounts for approximately eighty percent of the pulsatile impedance signal. During systole the aorta distends with ejected blood, creating a transient parallel low-resistance pathway that decreases total thoracic impedance, and it is this decrease, this fleeting dip in the impedance trace occurring roughly 60 milliseconds after aortic valve opening, that carries the hemodynamic information from which stroke volume can be derived.
Kubicek and colleagues at the University of Minnesota published the foundational stroke volume equation in 1966, modelling the thorax as a uniform cylinder filled with a homogeneous conductor:
SV = ρ × (L² / Z₀²) × (dZ/dt)_max × LVET
Every variable embeds an assumption whose adequacy can be questioned, and it is worth being precise about this because the analogy I want to draw from the technique depends on the precision of the substrate from which it is drawn. Blood resistivity (ρ) was fixed by Kubicek at 150 ohm-centimeters; later work by Quail and colleagues measured a mean in vivo value of 135 ± 1.0 ohm-centimeters at hematocrit 40%, and Mohapatra and colleagues showed in 1977 that assuming the standard 150 while ignoring patient hematocrit overestimates cardiac output by roughly 14.5% against radioisotope reference values, so that even the first variable in the equation is already an approximation whose adequacy depends on how much physiological variation one is prepared to absorb into a constant. L is the distance between the inner voltage-sensing electrodes, typically between the base of the neck and the xiphoid. Z₀ is the total quasi-static transthoracic base impedance, the parallel sum of everything that resists current flow when the heart is between beats, with typical adult values of 20 to 33 ohms. (dZ/dt)_max is the peak first derivative of the time-varying impedance signal, temporally coinciding with peak aortic blood flow acceleration. LVET, the left ventricular ejection time, is measured from the impedance waveform as the interval between aortic valve opening (the B-point) and aortic valve closure (the X-point).
Subsequent modifications have followed a characteristic pattern. Sramek replaced the uniform cylinder with a truncated cone in 1983 and absorbed blood resistivity into geometric constants; Bernstein added a dimensionless weight correction factor in 1986, then argued in a 2010 reanalysis that (dZ/dt)_max functions as an ohmic mean acceleration analog rather than a pure flow velocity surrogate. Woltjer and colleagues found in 1996 that the Sramek-Bernstein modification significantly underestimates stroke volume in obese patients while the original Kubicek method showed no weight bias. Each refinement absorbs one source of error and introduces another, so that the trajectory of the technique has been one of managed rather than eliminated approximation.
What concerns me is not the equation but an assumption underneath it that is, so far as I can determine, never explicitly stated in any foundational ICG paper. A measurement current is injected into the thorax, and the thorax contains, among other structures, the heart, an electrically active organ whose function depends on coordinated depolarization waves propagating through cardiac tissue at specific amplitudes and frequencies; the injected current contributes, however infinitesimally, to the electromagnetic environment of the thorax, which means that the measurement alters the system being measured. No anxiety attaches to this fact in the ICG literature, and for good empirical reasons: cardiac muscle membranes cannot depolarize in response to alternating current above roughly 500 hertz, and ICG operates at 20,000 to 100,000 hertz, which is 40 to 200 times above the ceiling for cardiac excitation; the 1 to 4 milliamperes of surface current distributes across the entire thoracic cross-section, producing field strengths at the myocardium on the order of nanovolts per centimeter against the heart’s endogenous field of roughly one millivolt per centimeter, a perturbation-to-signal ratio of approximately one part in a million. Even in the limiting case, where patients carry implanted cardiac electronic devices providing direct intracardiac conductors that would amplify any perturbation if one existed to amplify, a 2018 study by Borsali and colleagues (200 patients, pacemakers and defibrillators) found no significant changes in battery voltage, lead impedance, or pacing thresholds, and no inappropriate sensing events at six- and twelve-month follow-up. A rigorous formal proof of zero perturbation does not and cannot exist, because physics dictates that any current through a conductor creates some electromagnetic field, however vanishingly small, but the perturbation falls so far below any measurable or physiologically meaningful threshold that it is operationally zero.
It would be wrong to conclude from this that impedance cardiography is a precise technique; its imperfection is real, simply of a different kind than perturbation. A 1999 meta-analysis by Raaijmakers and colleagues, covering 154 validation studies across three decades, found a pooled correlation of r = 0.82 against reference methods, and more recent meta-analyses put the mean percentage error for absolute values at roughly 48% in adults against thermodilution, well above the clinically acceptable threshold of 30%; the ESCAPE BIG substudy found poor agreement between ICG and pulmonary artery catheter hemodynamic profiles in heart failure patients. ICG remains useful, nevertheless, for tracking relative trends, for determining which direction cardiac output is moving even when it cannot determine precisely where cardiac output is, and it fails in specifiable and well-characterized ways: arrhythmias eliminate the A-wave and produce beat-to-beat variability; pleural effusions corrupt the pulsatile signal; severe obesity distorts thoracic conductor geometry; sepsis, with its vasoplegia and capillary leak, violates the model’s assumptions about blood-tissue impedance contrast. Failure is graded rather than catastrophic, a progressive degradation of reliability as conditions push the ratio of the model’s assumptions to the thorax’s actual electromagnetic reality further from the favorable baseline.
Because the misuse of physics in philosophical writing has made me wary of contributing to it, a clarification: the self-perturbation structure I have described is not the Heisenberg uncertainty principle. σ_x · σ_p ≥ ħ/2 is a theorem about the intrinsic indeterminacy of quantum states, derivable from the non-commutativity of quantum observables, and has nothing to do with instrumental disturbance; the original gamma-ray microscope thought experiment unfortunately suggested a disturbative reading, but this has been rejected by physicists working on the foundations of quantum mechanics for decades. A thermometer absorbing heat from the liquid it measures, an ammeter altering current in the circuit it monitors, an impedance cardiograph injecting current into the thorax it interrogates: these are classical observer effects, perturbations that are in principle reducible and whose magnitude depends on the ratio of the measurement apparatus’s energy to the system’s own dynamics, and their philosophical interest is that they are more tractable and more pragmatically instructive than the quantum case, because the perturbation can be characterized, minimized, corrected for, and in some circumstances even exploited.
The analogy breaks at a specific point, and the break matters more than the correspondence. In impedance cardiography, the measuring instrument and the system being measured are ontologically distinct: the electrode array is not the heart; the injected current is not the cardiac cycle; the signal-processing chain that extracts (dZ/dt)_max inhabits a different causal order from the aortic blood flow it tracks. In introspection, this distinction collapses. When I attend to my own anxiety in order to characterize it, the attention and the anxiety are not separate systems; they are both activities of the same mind, drawing on the same finite pool of cognitive resources, and the “measurement current” is a reallocation of resources already internal to the system. Any attempt to model introspection on physical measurement must contend with this collapse, and the perturbation-to-signal ratio survives it only as a structural concept, not as a description of the same mechanism operating in a different domain. In impedance cardiography, perturbation is energetic: a current is added. In introspection, perturbation is attentional: cognitive resources are reallocated, and the reallocation changes the state being observed.
Introspective distortion has distinct forms, and conflating them, as both the philosophical literature and the therapeutic literature routinely do, obscures the conditions under which each operates. Attention directed at a mental state alters that state in real time; this is what James described when he compared introspection to catching a snowflake in the warm hand, the crystal becoming a drop, the transitive feeling becoming a substantive thing, the alteration simultaneous with the observation. Attention reorganizes cognitive resources, recruits working memory, engages prefrontal circuits that change the neural dynamics of the state being attended to, so that when I turn my attention to an incipient emotion to determine whether it is anger or grief, the attentional act itself changes the emotion’s valence and intensity, because attention reallocates the very resources that constitute the state. This is perturbation proper, the mechanism closest to the ICG case, and the degree of disruption scales with the intensity of attentional engagement, from casual noticing through focused examination to effortful verbal articulation.
But much of what passes for introspective access is not real-time perturbation at all; it is retrospective reconstruction, memory distorting past states in the act of retrieving them. When I report on what I felt during a clinical encounter an hour ago, I am constructing a plausible narrative from fragmentary cues, colored by my current mood, my theoretical commitments about what I should have felt, and the narrative conventions available to me. There is no real-time interaction between the measurement and the signal here; the corruption occurred before the reading began, more analogous to reading a damaged data file than to injecting current into a live system. Schwitzgebel’s dream-color case belongs in this category: the shift from black-and-white to color dream reports across the 1950s and 1960s is a reconstruction of past experience contaminated by culturally available categories.
External interpretive frameworks introduce a third structure of distortion, where the framework through which one observes imposes structure onto material that may have had no such structure before the framework was applied. Psychoanalytic suggestion, diagnostic categories that organize inchoate distress into named disorders, the vocabulary of cognitive distortions that CBT provides: Grünbaum’s 1984 critique identified this, showing that the analyst’s interpretive framework shapes what the patient produces, so that resistance, when a patient rejects an interpretation, is itself interpreted as confirming the interpretation’s accuracy, a loop in which a poorly calibrated instrument imposes its own frequency signature onto the signal.
Beyond perturbation, reconstruction, and contamination lies the possibility that certain features of one’s own mental life are not accessible to introspection, that self-knowledge has limits no refinement of technique can overcome, because the self exceeds its own capacity for self-apprehension. This is structural opacity, and it is the contribution of the Islamic philosophical tradition that I want to develop here.
I initially attributed the epistemological distinction between pre-reflective self-awareness and deliberate introspective examination to al-Fārābī, and this turns out to be wrong, or at best imprecise. In the Risāla fī al-ʿAql the intellect achieves self-intellection only at its highest stage of development, when, having accumulated intelligibles through knowing external objects, it becomes its own object through the principle that the knower becomes identical with the known; the reflexive meta-cognitive condition that certitude must include knowing-that-one-knows is genuine (Deborah Black identifies it as among al-Fārābī’s innovations in a 2006 article on his epistemology), but it does not amount to a theory of pre-reflective self-awareness as a distinct epistemic category. As Black put it in a conversation with Peter Adamson, the inclusion of introspective knowledge among the foundations for knowledge “is something I don’t think that Fārābī really considered to be an important or even perhaps he didn’t even entertain that as a possible philosophical method.” What one gets from the Fārābian corpus is the Aristotelian backdrop, self-intellection through cognitive identity and knowing-that-one-knows as a condition of certitude, against which the Avicennian innovation becomes visible.
Consider the thought experiment: a fully formed adult created suspended in void, limbs spread apart, all sensory input blocked. Would this person be aware of their own existence? Ibn Sīnā’s answer is yes: the person would affirm the existence of their self (wujūd dhāti-hi) even without any sensory, imaginative, or reflective content. This is al-shuʿūr bi-al-dhāt, awareness of the self, and Black’s analysis of the Avicennian texts identifies its essential features: it is not acquired from outside, requires no instrument or medium, is present from the soul’s inception, is continual rather than intermittent, and is identical with the self’s existence rather than being a separate cognitive act directed at it. One is always self-aware, even when asleep or attending to something else entirely, and one is often not aware of being self-aware, a paradox only if one assumes that awareness must involve attentional focus. Against this primitive, continuous self-presence stands a second, intermittent level: reflexive self-awareness, the deliberate turning of attention onto one’s own mental states, knowing-that-one-knows in the Fārābian sense but now treated as an epistemically distinct and potentially distorting operation rather than a simple meta-cognitive addition. In the Mubāḥathāt the formulation is compressed to the point of near-opacity: the awareness of self-awareness is different from self-awareness.
The temptation is to map this two-tier framework directly onto the ICG apparatus, with al-shuʿūr bi-al-dhāt as the base impedance Z₀ and deliberate introspection as the measurement current. The mapping is suggestive but imprecise. Z₀ is measurable, stable, and quantifiable; pre-reflective self-awareness is none of these things. It is a phenomenological condition posited to explain the possibility of self-knowledge, not an observable parameter that could be read off an instrument. The correspondence is structural, not substantive: both are background conditions that persist independently of any deliberate probe, and both are altered (or at least potentially altered) when a measurement is introduced. The analogy tracks the relationship between baseline and probe, not the nature of either term.
If one asks what kind of perturbation is at stake when the probe is introduced, the sharpest epistemological formulation comes from the Ishrāqī tradition. ʿIlm al-ḥuḍūrī (knowledge by presence), developed primarily in Suhrawardī’s Ḥikmat al-Ishrāq, holds that self-knowledge is paradigmatically direct, the self present to itself without any representational intermediary, which avoids the infinite regress that would follow from requiring a mental representation of the self to know the self (one would then need a representation of the representation, and so on); ʿilm al-ḥuṣūlī (knowledge by representation), by contrast, requires an abstracted form of the object, introducing a mediating structure between knower and known. The distinction identifies language and conceptualization as the mediating structure: when one moves from pre-reflective awareness of an emotion to a reflective judgment that “I am anxious,” the judgment introduces a representational form (the concept anxiety, drawn from a cultural and diagnostic vocabulary) that discretizes what may have been continuous, names what may have been ambiguous, and fixes what may have been in flux. The “injected current” of introspection, then, is the representational apparatus that attention recruits, the conceptual and linguistic scaffolding through which raw experience must be translated to become an object of knowledge.
Whether the self is fully transparent to itself even in presential knowledge, or whether there exists an irreducible opacity, received its most consequential treatment in the Ṣadrāʾī synthesis. Ittiḥād al-ʿāqil wa-l-maʿqūl (unity of the knower and the known), where knowledge is an existential transformation of the knower’s mode of being, would seem to resolve the perturbation problem entirely, since the knower and known are not distinct entities that could perturb each other; but Kaukua, in a 2014 article, argues that Mullā Ṣadrā holds that full knowledge of one’s own essence remains partially inaccessible. Self-opacity, on this reading, is closer to a bandwidth limitation than to a failure of any particular introspective technique: a mismatch between the complexity of what one is and the capacity of any single introspective act to capture it. Whether this maps as cleanly onto the ICG performance data (the pooled r = 0.82 for trends against a 48% mean percentage error for absolute values) as I initially supposed is, on reflection, uncertain; the correspondence is suggestive rather than demonstrative, because ICG’s absolute-value error arises from geometric and physiological model assumptions while Ṣadrā’s opacity arises from metaphysical features of selfhood. What the two cases share is the asymmetry between directional reliability and absolute precision, and I am inclined to treat this as a structural isomorphism worth taking seriously without claiming it is more than structural.
In the Western tradition the perturbation problem in introspection was discovered independently and later. Innere Wahrnehmung (inner perception, a structural, always-on awareness of one’s own mental acts, functioning en parergo, on the side) and innere Beobachtung (inner observation, which would require turning the mental act into one’s primary attentional object and thereby altering or destroying it) are Brentano’s terms, from Psychology from an Empirical Standpoint (1874), and they map precisely onto the Avicennian distinction, a cross-traditional resonance that owes nothing to historical transmission and everything to the structure of the problem constraining the range of available solutions.
Introspection directed at the transitive states of consciousness, the feelings of relation, of tendency, of movement-toward, produced James’s most precise articulation of the perturbation problem in The Principles of Psychology (1890): the comparison to seizing a spinning top to catch its motion, or trying to turn up the gas quickly enough to see how the darkness looks; and more precisely, the observation that as a snowflake crystal caught in the warm hand is no longer a crystal but a drop, so, instead of catching the feeling of relation moving to its term, we find we have caught some substantive thing, where the warm hand is the attentional-representational apparatus, the crystal the labile state, and the drop what survives translation into a form the reflective mind can hold.
Circularity in self-perturbing measurement systems has received rigorous treatment in Chang’s Inventing Temperature (2004), where the deep circularity of thermometry (calibrating a thermometer requires knowing the temperature, but knowing the temperature requires a calibrated thermometer) is resolved through iterative epistemic bootstrapping: knowledge advancing through cycles of imperfect measurement guiding theory, which in turn improves measurement. A thermometer absorbs heat from the body it measures; the perturbation is never zero; scientists developed techniques to minimize and correct for it without ever eliminating it, and the process of successive refinement, of imperfect instruments tested against imperfect but improvable standards, is itself a form of knowledge production. Within this framework the perturbation component of introspective distortion (the reconstruction, contamination, and opacity components have different structures and do not respond to the same remedies) becomes epistemically tractable: the question is not whether the perturbation is zero but whether the perturbation-to-signal ratio is small enough, and characterizable enough, that the output still carries information about the system as it was before the measurement began.
Whether introspective perturbation is necessary or merely conditional determines whether this amounts to a philosophical claim or a pragmatic observation. In impedance cardiography, perturbation is necessary: the technique cannot function without injecting current, and injecting current necessarily alters the electromagnetic environment; the perturbation is operationally negligible, but it is not zero, and it cannot in principle be made zero because the measurement is the perturbation. In introspection, the case is less clear. If one accepts the Suhrawardian framework, presential self-knowledge involves no representational intermediary and therefore no perturbation; it is only when one moves to representational knowledge, to the deliberate articulation and categorization of experience, that the mediating apparatus introduces distortion. On this view, perturbation is conditional: it arises from a specific kind of introspective operation (representational, linguistic, categorizing) rather than from introspection as such. Pre-reflective self-awareness, the Avicennian al-shuʿūr bi-al-dhāt, is the limiting case of zero-perturbation introspection, analogous to a hypothetical measurement that reads the impedance without injecting any current, which is physically impossible in the ICG case but may not be epistemically impossible in the introspective case.
The argument is conditional: when introspection recruits the representational, linguistic, and conceptual apparatus required to produce propositional self-knowledge that can be communicated, assessed, or acted upon, it introduces a mediating structure that alters what it mediates, and the degree of alteration scales with the weight of the apparatus recruited, from casual noticing at one end of the spectrum through focused examination and verbal articulation to articulation for a grading audience, under duress, in temporal proximity to the experience being examined, at the other.
The therapeutic and educational deployment of introspection, read through this framework, resolves into a collection of distinct measurement instruments, each recruiting different amounts of representational apparatus, each therefore operating at a different perturbation level, and each valid only under conditions that keep the perturbation-to-signal ratio favorable.
Free association is vulnerable to the specific perturbation that Grünbaum’s 1984 critique identified, but the mechanism is contamination rather than perturbation proper: the analyst’s interpretive framework shapes what the patient produces, imposing structure onto material that may not have had that structure prior to the analytic encounter. Resistance is the sharpest case, because when a patient rejects an interpretation the rejection is itself interpreted as confirming the interpretation’s accuracy, creating a loop in which the instrument’s frequency signature dominates the output.
Structured introspective instruments of the kind that cognitive behavioral therapy employs (thought records, cognitive distortion logs) operate through perturbation proper: they require the patient to attend to, name, categorize, and evaluate cognitions in real time, recruiting heavy representational apparatus. Focusing on thought content, even to challenge it, may inadvertently reinforce the engagement with negative cognitions that constitutes the pathology; this is the core of Wells’s metacognitive critique, and Wegner’s ironic process theory provides the mechanism, because the automatic monitoring required to check whether an unwanted thought is present keeps the thought active, establishing a recursive loop that alters the frequency and character of the cognitions the instrument claims to passively observe.
Expressive writing complicates the picture because the research originating with Pennebaker suggests that perturbation is sometimes the therapy itself: benefit requires constructing new meaning rather than recounting events; subjects whose function words changed most from day to day showed the greatest improvement while those who began with a coherent story generally did not benefit, which implies that journaling works precisely when the representational apparatus changes how one holds the experience, when the mediating structure transforms. Between therapeutic perturbation and counterproductive rumination the difference is real but not always visible from inside the process, which is itself evidence that introspective access to the quality of one’s own introspection is limited, a second-order instance of the opacity problem.
One failure mode I have encountered as a professional obligation deserves separate treatment. Residency programs in the United States mandate, through the ACGME’s six core competencies adopted in 1999 and operationalized through the Milestones framework, that trainees identify strengths, deficiencies, and limits in their knowledge and expertise; the Common Program Requirements specify “self-assessment and reflection”; narrative medicine, formalized through Charon’s program at Columbia, adds close reading, reflective writing, and creative writing to the curriculum; reflective portfolios are graded. A 2019 article in Perspectives on Medical Education introduced the concept of the reflective zombie, adapting Chalmers’s philosophical zombie, to name someone who displays all the outer traits of reflection without having reflected; the authors argued that operationalizing reflection for assessment has discarded its philosophical foundations, and that externalization changes the nature of private reflection because there is now an audience.
But the problem is more specific than performative inauthenticity, and it involves every form of distortion simultaneously. A medical trainee asked to reflect on her learning while sleep-deprived, while processing more clinical information than working memory can hold, while carrying the emotional residue of a death she may or may not have contributed to, and while facing a graded assignment requiring her to demonstrate insight into her own performance, is in a situation where the attentional perturbation is maximal because she must recruit heavy representational apparatus under conditions of cognitive resource depletion, where the reconstruction is unreliable because she is reporting on recent experience with inadequate temporal distance, where the contamination is systematic because she knows what a “good reflection” looks like and will produce one, and where she is being asked about surface-level performance that she cannot reliably access even under favorable conditions. The resulting output, which will look and read and be graded as a reflection, measures her capacity to generate introspective output under conditions where genuine introspection is not possible. ICG specifies its contraindications: arrhythmia, pleural effusion, severe obesity, sepsis. Reflective practice mandates its technique in precisely the conditions most likely to produce artifacts and then interprets the artifacts as data.
Introspection is a measurement technique that, like all measurement techniques, perturbs the system it measures, but the perturbation is conditional rather than necessary: it arises when introspection recruits representational apparatus (language, concepts, categories, evaluative frameworks) and scales with the weight of that apparatus. Pre-reflective self-awareness, in the Avicennian framework, is the limiting case of perturbation-free self-knowledge, continuous and self-generating, requiring no representational mediation; deliberate introspection is the measurement that introduces mediation, valuable because it extracts communicable, actionable knowledge that pre-reflective awareness cannot provide, but carrying the cost of an introduced structure whose effects must be monitored. Presential knowledge, in the Ishrāqī formulation, specifies the nature of the cost: the transition from presence to representation, from ḥuḍūrī to ḥuṣūlī, is the moment at which the mediating apparatus enters the circuit. And the Ṣadrāʾī opacity thesis sets the outer boundary of what even the lightest representational apparatus can achieve, because beyond the perturbation and the reconstruction and the contamination there remains a residual inaccessibility that is structural rather than instrumental.
In practice, what this amounts to is a principle of introspective restraint that I have never seen stated in the medical education literature though it is implicit in the physics: measure when the perturbation-to-signal ratio is favorable, when one is relatively calm, when the audience is oneself, when the temporal distance from the experience is sufficient to minimize reconstruction error, when the representational apparatus one recruits is light rather than heavy; do not trust the measurement when the ratio is unfavorable, under duress, for an audience, on demand, in the acute phase of the experience one is trying to examine; distinguish perturbation from reconstruction from contamination from opacity, because they have different structures and different remedies; and trust the trends more than the absolute values, because one knows which direction one is moving even when one is probably wrong about exactly where one is. If one is honest about the cost of the current, one will measure less often, more carefully, and with less confidence in the absolute values than in the direction of change, which is what matters in both cardiology and conscience.
Selected Bibliography and Readings



Leave a comment